

Introduction:
Plasma cell neoplasms can show aberrant expression of different lineages related antigens, but expression of T-cell associated markers, is exceedingly rare. Herein, we describe two patients with plasma cell Myeloma who relapsed with an aggressive disease with plasmablastic morphology, skin involvement, high Ki-67, complex karyotype (with abnormalities in chromosome 1) and interestingly both patients showed aberrant acquisition of single or multiple T-cell associated markers including CD4 and died shortly after last presentation. T-cell markers were not expressed at diagnosis. Multiple theories have been proposed to explain aberrant expression of T-cell markers on a terminally differentiated plasma cells. Due to rarity of this aberrant phenotype and scarcity of the published data, the precise causative mechanism and its clinical implications have not yet been elucidated. An extensive literature review for patients with similar findings was conducted and the relevant pathological, clinical and prognostic characteristics were summarised.
Methodology:
Herein we describe two patients with emergent plasmablastic morphology and aberrant acquisition of multiple T‐cell markers (confirmed by both flow cytometry (FCM) and immunohistochemistry), diagnosed in national Centre for Cancer Care and Research in Qatar. In addition, we conducted a systematic literature review using PubMed, google scholar and Scopus for patients with plasma cell myeloma (PCM) and aberrant T-cell expression, using pre-defined search terms and synonyms.
Results:
Patients diagnosed in our centre:
Case 1:
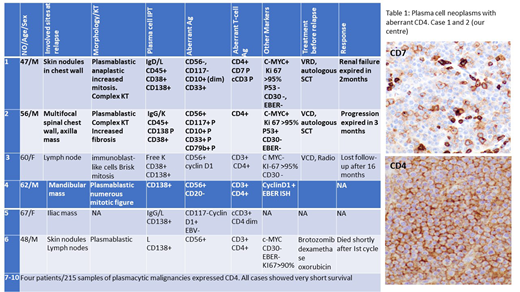
A 47-year-old male presented with multiple subcutaneous swellings, skin biopsy showed plasma cell neoplasm (PCN). Serum protein electrophoresis showed two bands; IgD lambda and free lambda. The patient started on VRD followed autologous SCT. Two months later, he developed new skin nodules in the upper chest wall and right renal mass.
BM at relapse, showed many pleomorphic myeloma cells with plasmablastic/ anaplastic morphology. FCM showed a large population of monotypic plasma cells expressing CD10 with aberrant expression of CD33, CD4 and CD7 (partial). By IHC: the plasma cells were positive for cMYC with aberrant expression of CD4 and CD7 (partial) and CD3 (minority of cells) with Lambda light chain restriction and negative for CD20, CD56 and CD117. KI-67 >90%. Karyotype: 47,X, Y,i(1)(q10) ,t(1;3)(p32;p13),+der(3)t(1;3)(p32;p13) ,add(4)(q35),der(8)t(8;15)(q24;q11.2) add(8)(p23),add(13)(q34),+20[20].
The patient started on second line treatment for two days, unfortunately, he progressively deteriorated and passed away.
Case 2:
56-year-old male presented with solitary spinal plasmacytoma and PCM. The patient underwent local radiotherapy followed by Lenalidomide and dexamethasone for 12 cycles and achieved complete remission. 5 years later, the disease progressed with multifocal spinal lesions and right chest wall mass which was treated with Pomalidomide and Daratumumab but he progressed and developed as scalp mass lesion.
BM was infiltrated by many myeloma cells with plasmablastic morphology. FCM showed a monotypic plasma cell with aberrant expression of CD4 and complex karyotype. New line of therapy include Elotuzumab-Pomalidomide-dexamethasone started and unfortunately the patient shortly succumb.
Upon literature review:
A total of 19 cases of PCNs (table 1) showed aberrant expression of T-cell associated markers (including the two cases reported here). 11 case at relapse & two at initial presentation. Anaplastic/plasmablastic morphology and extramedullary presentation were reported in 8/12 cases. 10/18 patients out showed aberrant expression of CD4. 9/11 cases had a very short survival.
Conclusion:
Here we discuss an interesting, yet a rare finding of aberrant acquisition of T-cell associated markers on PCM. This review emphasises the importance of recognising atypical and rare immunophenotypic aberrancies in PCN that could possibly lead to diagnostic pitfalls (particularly with extramedullary involvement) and provide important prognostic information.
We conclude that there is an evident association between aberrant expression of T-cell associated markers on PCM and aggressive disease including plasmablastic morphology, high KI-67, extramedullary involvement and adverse outcome with short survival.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal